
A Practical Guide to Workplace Stress for UK Employers
Workplace stress can damage wellbeing, performance, and organisational resilience. This guide explains the causes, signs, legal responsibilities, and practical steps UK employers can take to manage stress more effectively.

What It Is, What It Does to the Body, and What Every UK Employer Is Required to Do
Workplace stress is one of the most significant and most mismanaged health risks in the UK today. Nearly a million workers reported work-related stress, depression or anxiety in 2024/25, a record high, and the financial cost to employers runs to tens of billions of pounds annually. Yet the response from most organisations remains reactive, superficial, or both.
This guide is an attempt to do the subject properly. It examines what stress actually is, where the concept came from, what it does to the body over time, what the law requires of UK employers, and what evidence-based intervention looks like. If you are an HR manager, a line manager, an employer, or someone trying to understand why stress has become such a dominant feature of working life, this is written for you.
The Scale of the Problem: UK Stress Statistics
The Health and Safety Executive (HSE) publishes annual figures on work-related ill health. The most recent data, published in November 2025 and covering 2024/25, represents a record high.1
964,000
workers with work-related stress, depression or anxiety (2024/25)
22.1m
working days lost to stress, depression and anxiety
52%
of all work-related ill health attributed to stress
62%
of all working days lost due to work-related ill health
22.9 days
average absence per stress case (vs 7 days for physical injury)
+24%
increase in cases from 2023/24 to 2024/25
To put the trajectory in context: in 2023/24 there were 776,000 cases and 16.4 million days lost. In a single year, cases rose by approximately 188,000 and days lost by nearly 6 million. Stress, depression and anxiety now account for more than half of all work-related ill health in Great Britain, and nearly two thirds of all working days lost to work-related ill health.
The financial cost compounds the human one. Analysis by Deloitte found that poor mental wellbeing costs UK employers an estimated £51 billion a year, with presenteeism alone accounting for £24 billion of that figure.2 At the national level, the Mental Health Foundation and the London School of Economics and Political Science calculated that poor mental health costs the UK economy £117.9 billion annually, equivalent to around 5% of GDP.3
Survey data adds further texture. The Mental Health UK Burnout Report 2025, based on a YouGov survey of nearly 4,500 UK adults, found that nine in ten respondents had experienced high pressure or stress in the past year.4 This is a survey finding rather than a hard national prevalence figure, but it is consistent with the HSE data in indicating that stress is not a marginal experience. Around one in five workers reported needing time off due to poor mental health caused by stress.
What Stress Actually Is: A Brief History of the Concept
The word "stress" did not enter medical or psychological vocabulary until the early twentieth century. Its roots are in physics, where it described the internal distribution of a force acting on a material body, producing what engineers call strain. Understanding how it migrated from structural mechanics to human experience matters, because it shapes how we still think about the concept today, and why so much confusion surrounds it.
Claude Bernard and the Internal Environment
The intellectual foundations begin in 1865 with the French physiologist Claude Bernard, whose Introduction to the Study of Experimental Medicine introduced the concept of the milieu intérieur: the stable internal environment that an organism must maintain to survive. Bernard observed that living systems constantly work to keep their internal conditions within acceptable ranges despite external fluctuations. This insight, that life is an ongoing project of internal regulation, became the bedrock on which all subsequent stress research was built.5
Walter Cannon and the Fight-or-Flight Response
The next major contribution came from the Harvard physiologist Walter Cannon. Working in the early twentieth century, Cannon formalised Bernard's concept into what he called homeostasis: the body's tendency to maintain physiological stability through continuous, active regulation.6 In 1915 he described the fight-or-flight response: a set of coordinated physiological reactions triggered when an organism perceives a threat. Heart rate increases, blood is redirected from the digestive system to the muscles, breathing quickens, glucose is released into the bloodstream, and the pupils dilate. These reactions are mediated by the sympathetic nervous system and adrenaline, and they exist for one purpose: to mobilise the body for rapid physical action.
Cannon's insight was that this response is adaptive. A genuine physical threat demands an immediate, full-body commitment to either fighting or running. The problem, which Cannon also recognised, is that the same response fires when no physical threat is present: when the perceived danger is a performance review, a difficult conversation with a manager, or an urgent email about quarterly targets. The body's alarm system responds to perceived threat, not to the actual nature of that threat, which is why modern working life generates so much physiological wear.
Hans Selye and the General Adaptation Syndrome
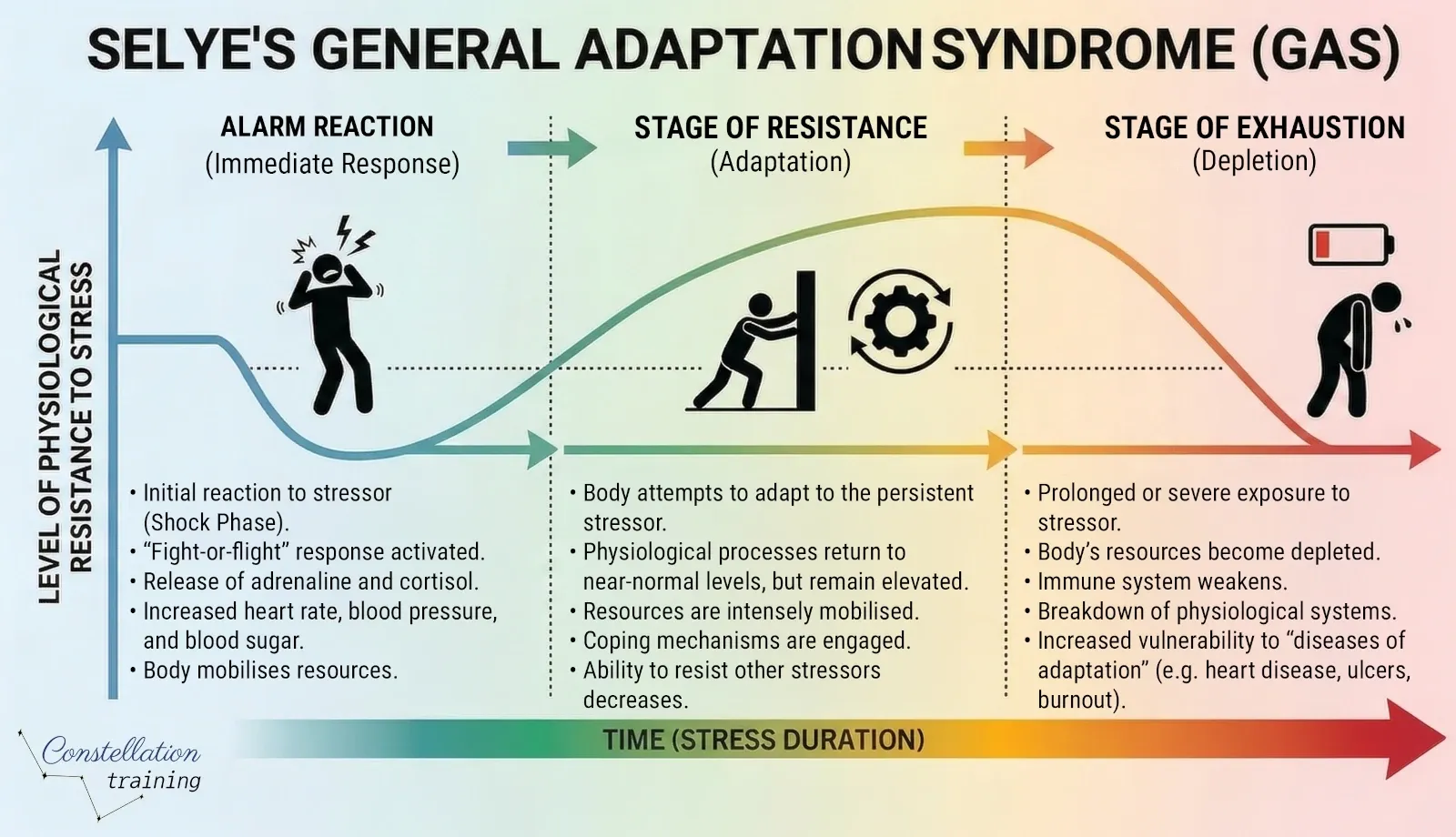
The endocrinologist Hans Selye is most responsible for bringing "stress" into common usage. Working at McGill University in the 1930s, he noticed that rats subjected to very different harmful stimuli, cold, surgical injury, toxic injections, showed the same physical changes regardless of the specific cause: enlarged adrenal glands, shrunken lymphatic tissue, and gastric ulcers.7 Selye concluded that the body had a universal, non-specific response to any demand placed upon it. He called this the General Adaptation Syndrome (GAS), describing it in three phases.
| Stage | What Happens |
|---|---|
| Alarm Reaction | The initial shock response. Adrenaline and cortisol flood the system. The sympathetic nervous system activates and resources are mobilised. This is Cannon's fight-or-flight in action. |
| Stage of Resistance | The body adapts and attempts to cope. The acute physiological reactions partially subside but the organism remains on heightened alert, burning through reserves to maintain the response. |
| Stage of Exhaustion | If the stressor continues, the body's adaptive resources are depleted. This is where chronic disease risk accumulates: immune suppression, cardiovascular strain, and psychological breakdown. |
Selye also introduced a distinction that remains useful: eustress (positive, motivating stress) versus distress (harmful, overwhelming stress). A job interview, a sporting challenge, a creative deadline can produce the same physiological arousal as negative stressors, but with different cognitive appraisal and different outcomes. Not all stress is damaging. It is chronic, unmanaged distress that causes harm.8
Modern Understanding: Cognitive Appraisal and Individual Differences
Selye's model was influential but incomplete. Later researchers, particularly Richard Lazarus in the 1960s and 1970s, demonstrated that the stress response is not purely automatic. What matters is how an individual appraises a situation: whether they perceive it as threatening, whether they believe they have the resources to cope, and what the stakes appear to be. Two people in the same meeting can have entirely different physiological and psychological responses to the same news, based on personal history, current resources, and cognitive framing. This explains why stress cannot be managed purely at the level of the stressor. Resilience, perception, social support, and individual coping strategies all shape the relationship between pressure and harm.
What Stress Does to the Body and Mind
Being precise about the mechanisms matters. It explains why chronic stress produces such a wide range of physical and psychological symptoms, and why the consequences of untreated workplace stress extend well beyond feeling anxious at your desk.
The Physiological Cascade
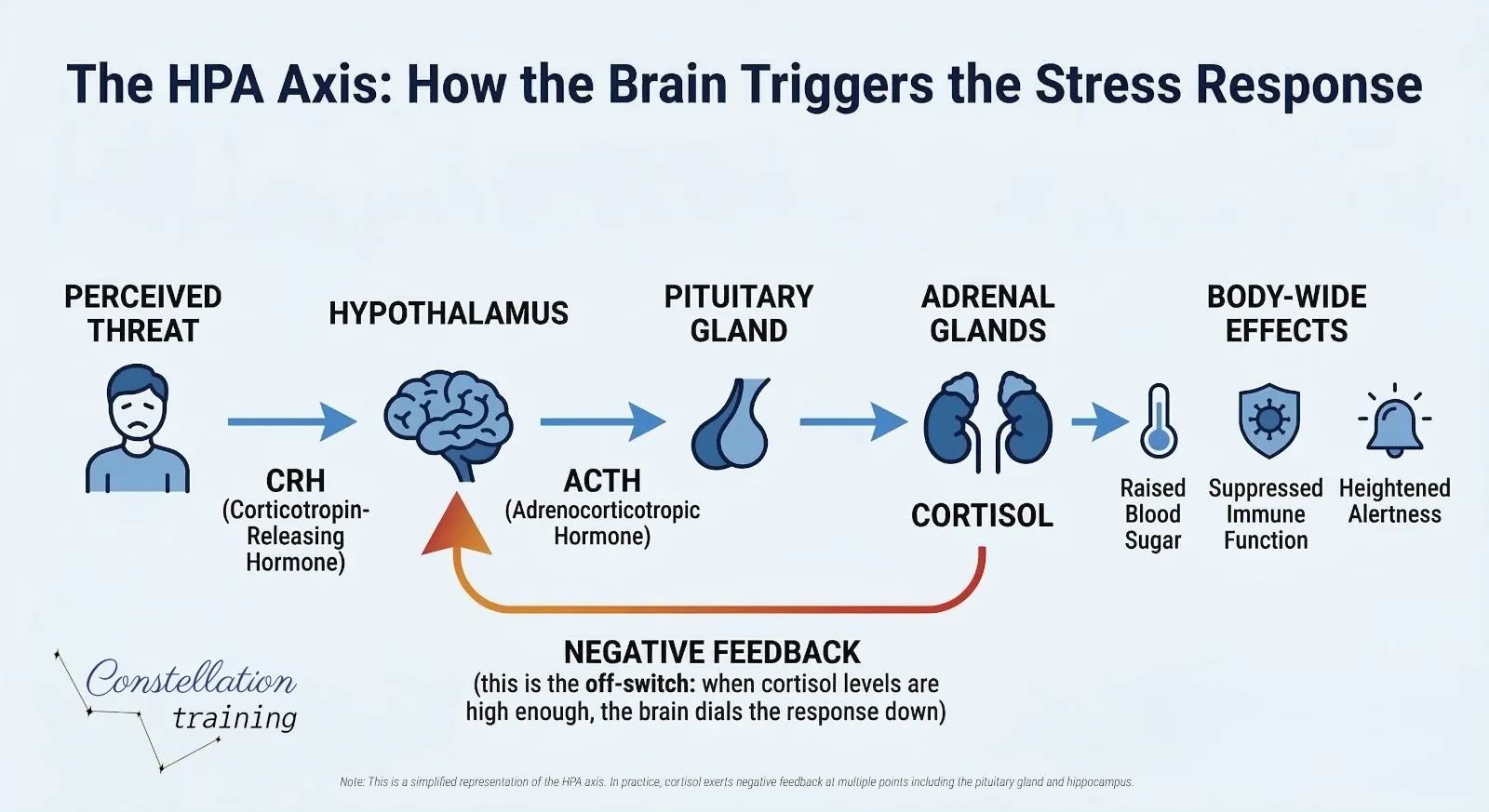
When the brain detects a stressor, real or perceived, the hypothalamus activates two overlapping response systems simultaneously.
The first is the sympatho-adrenal system. The hypothalamus signals the adrenal medulla to release adrenaline and noradrenaline. These hormones produce immediate effects: accelerated heart rate, raised blood pressure, rapid breathing, pupil dilation, muscle tension, and suppression of non-emergency functions such as digestion and immune activity.
The second is the hypothalamic-pituitary-adrenocortical (HPA) axis. The hypothalamus triggers the pituitary gland to release adrenocorticotrophic hormone (ACTH), which signals the adrenal cortex to produce cortisol. Cortisol is the primary long-acting stress hormone. It increases blood glucose, suppresses immune activity, and affects brain function. This pathway is slower to activate but slower to resolve, making it particularly important in chronic stress.9
What Prolonged Stress Does
A stress response designed for brief, intense situations becomes destructive when it runs continuously. The effects accumulate across multiple body systems.
Cardiovascular: Sustained elevated blood pressure and repeated surges in adrenaline are associated with increased cardiovascular risk, including accelerated arterial damage and greater susceptibility to heart disease.
Immune: Prolonged cortisol suppresses immune function, increasing vulnerability to infection, slowing wound healing, and contributing to persistent fatigue.
Digestive: Stress diverts blood away from the gut and suppresses digestive function. Chronic stress is associated with irritable bowel syndrome, gastric discomfort, and exacerbated inflammatory conditions.
Neurological: Sustained cortisol exposure is associated with changes in the hippocampus, the brain region central to memory and learning. This underlies the cognitive symptoms of chronic stress: poor concentration, memory difficulties, and impaired decision-making.
Sleep: Elevated cortisol disrupts the natural daily cortisol rhythm, interfering with sleep architecture. Sleep deprivation then compounds the stress response, creating a reinforcing cycle.
Mental health: Chronic activation of the stress response is strongly associated with anxiety disorders and clinical depression. The relationship is bidirectional: stress drives mental ill health, and mental ill health amplifies the stress response.
Psychological and Behavioural Symptoms
Alongside the physiological effects, chronic stress produces a recognisable cluster of psychological and behavioural changes. The HSE identifies the following as common indicators of work-related stress.
Psychological symptoms include anxiety, irritability, low mood, difficulty concentrating, feeling overwhelmed, poor judgement, loss of confidence, and persistent negative thinking.
Physical symptoms include headaches, muscle tension and pain, fatigue, sleep disturbance, gastrointestinal symptoms, and recurrent minor infections.
Behavioural changes include withdrawal from colleagues, reduced quality of work, increased errors, reliance on alcohol or other substances, increased absence, and presenteeism. The absence of obvious symptoms does not mean stress is absent, which is particularly relevant for managers tasked with understanding how their teams are coping.

Stress and the Wider Picture: Burnout, Anxiety, and Depression
Stress is frequently discussed alongside burnout, anxiety and depression as though they are interchangeable. They are not. Understanding the distinctions matters both for accurate identification and for choosing the right response.
Stress and Burnout
Burnout was classified by the World Health Organization in ICD-11 as an occupational phenomenon characterised by three dimensions: exhaustion or energy depletion, increased mental distance or cynicism about the job, and reduced professional efficacy.10 Burnout is generally understood as the end state of chronic, unmanaged workplace stress. The Mental Health UK Burnout Report 2025 found that nine in ten respondents had experienced high pressure or stress in the past year, and that burnout is a gradual process frequently mistaken for stress, depression, or anxiety, meaning it often goes unrecognised until the individual has been significantly harmed.
Stress, Anxiety, and Depression
Stress is typically a response to an identifiable external pressure and tends to resolve when that pressure reduces. Anxiety is characterised by persistent worry and fear that may continue in the absence of identifiable stressors. Depression involves sustained low mood, loss of interest, and a range of physical and cognitive symptoms that impair daily functioning.
Chronic stress can trigger and exacerbate both anxiety and depression, partly through the sustained effects of cortisol on brain function, and partly through the cumulative impact of exhaustion, helplessness and loss of control that unmanaged stress produces. Managing stress effectively is therefore also a primary prevention strategy for anxiety and depressive disorders, not a separate concern.
The Causes of Workplace Stress: What the Evidence Shows
The HSE identifies six primary categories of work design that, if poorly managed, produce stress. These are codified in the HSE Management Standards, a framework developed from large-scale research and introduced in 2004 as a practical tool for employers. Understanding these categories is essential to targeting intervention effectively rather than reaching for generic wellness programmes.11
| HSE Management Standard | What It Covers |
|---|---|
| Demands | Workload, work patterns, and the physical work environment. Stress arises when demands consistently exceed the individual's capacity to cope within available time and resources. |
| Control | How much say people have over the way they do their work. Low control over pace, priorities, and working methods is a well-established stressor. |
| Support | Encouragement, resources, and information from the organisation, line management, and colleagues. Inadequate support is particularly damaging during periods of high demand. |
| Relationships | Promoting positive working relationships and addressing unacceptable behaviour, including bullying, harassment, and conflict. |
| Role | Whether people clearly understand their role and whether the organisation ensures they do not have conflicting responsibilities. Role ambiguity is a significant and often overlooked stressor. |
| Change | How organisational change, large or small, is communicated and managed. Poorly managed change creates uncertainty, reduces trust, and generates sustained anxiety. |
The 2024/25 HSE data confirms these categories in practice. Workers most frequently cited workload, tight deadlines, and excessive pressure or responsibility as primary drivers, alongside lack of managerial support, organisational change, and role uncertainty.12
Who Is Most Affected
Stress is not evenly distributed. The HSE data consistently shows elevated rates in public administration and defence, human health and social work, and education. Workers in these sectors face a combination of high emotional demands, limited control, role complexity, and frequently insufficient resources.
The 2024/25 HSE statistics show that female workers report work-related stress, depression or anxiety at a rate approximately 25% higher than their male counterparts: 3,220 cases per 100,000 female workers compared with 2,580 per 100,000 male workers.13 Women aged 25 to 34 are in the highest-prevalence bracket, with elevated rates continuing through the 35 to 44 age group, a period when many women are managing combined work and caring responsibilities. Workers aged 18 to 24 are most likely to take time off due to poor mental health.
Frontline managers represent a particularly vulnerable group across all sectors. They absorb pressure from above and below simultaneously, are often inadequately trained for the people-management aspects of their role, and may feel unable to acknowledge their own difficulties without appearing unable to cope.
The Legal Framework: What UK Employers Are Required to Do
The legal requirements for UK employers on stress are clear, enforceable, and frequently misunderstood. Framing stress management as a wellbeing initiative or an optional extra reflects a fundamental misunderstanding of the law.
The Health and Safety at Work etc. Act 1974
Section 2 of the Health and Safety at Work etc. Act 1974 places a duty on every employer to ensure, so far as is reasonably practicable, the health, safety and welfare of all employees.14 The HSE has confirmed that "health" in this context includes psychological health. There is no legal distinction between physical and psychological harm. An employer who ignores a significant and foreseeable risk of psychological harm is in breach of the same duty as one who ignores a risk of physical injury.
The Management of Health and Safety at Work Regulations 1999
Regulation 3 of the Management of Health and Safety at Work Regulations 1999 requires employers to make a suitable and sufficient assessment of risks to employees' health and safety.15 This explicitly includes psychosocial risks. Employers therefore have a legal duty to assess and manage the risks of work-related stress, just as they would for manual handling or exposure to harmful substances. The HSE Management Standards provide a recognised framework for doing so.
The Equality Act 2010
Where stress contributes to or results from a mental health condition that meets the threshold of a disability under the Equality Act 2010, additional duties apply. Under the Act, disability means a physical or mental impairment that has a substantial and long-term adverse effect on a person's ability to carry out normal day-to-day activities. Where that threshold is met, employers may be required to make reasonable adjustments.16 Anxiety disorders, clinical depression, and PTSD exacerbated by workplace conditions can all meet this threshold. Failure to make appropriate adjustments constitutes disability discrimination.
Employers have a legal duty to assess and manage the risks of work-related stress under the Health and Safety at Work etc. Act 1974 and the Management of Health and Safety at Work Regulations 1999.
The HSE can investigate and take enforcement action against employers who fail to manage these risks. In December 2025 the HSE served a Notice of Contravention on a major UK university for failing to have effective arrangements in place to manage work-related stress.
Employees may, in some circumstances, bring civil claims for psychiatric injury where work-related stress was reasonably foreseeable and not properly addressed. Such claims turn on foreseeability, breach, causation, and evidence.
Where a mental health condition meets the disability threshold under the Equality Act 2010, additional duties to make reasonable adjustments apply.
What the Legal Duty Requires in Practice
Discharging the duty to assess and manage psychosocial risks using the HSE Management Standards approach involves the following steps.
- Gathering data on the six stressor areas, using the HSE Stress Indicator Tool (a 35-item staff survey), alongside absence data, return-to-work interviews, and exit interview information.
- Analysing the data to identify where conditions fall below the Management Standards thresholds.
- Running focus groups or consultation sessions to explore identified issues and develop targeted interventions.
- Implementing, recording, and communicating the agreed actions.
- Monitoring, reviewing, and updating the assessment as circumstances change.
The assessment must be documented and must specify the measures taken to address identified risks. The duty is ongoing, not a box-ticking exercise conducted once.
What Works: Evidence-Based Approaches to Managing Workplace Stress
There is a substantial body of evidence on what actually reduces workplace stress. Critically, the evidence distinguishes between interventions that address the causes (primary), those that build individual coping capacity (secondary), and those that treat people once harm has occurred (tertiary). All three levels matter, but the emphasis in too many organisations is heavily skewed towards the tertiary: employees become symptomatic, they access an Employee Assistance Programme, they may return to unchanged conditions. This is stress treatment, not stress management.
Primary Interventions: Addressing Causes at Source
Primary interventions target the organisational and job design factors that generate stress. They are the most effective category because they remove or reduce the hazard itself.
- Workload management: realistic job design, adequate staffing, and clear prioritisation. Where workload genuinely cannot be reduced, that conversation needs to be honest rather than aspirational.
- Autonomy and control: giving employees genuine say over how they work. Research consistently shows that high demand combined with low control is among the most damaging combinations.
- Role clarity: clear job descriptions, regular one-to-ones to clarify expectations, and explicit discussion of priorities. Role conflict, where employees receive incompatible demands from different managers, should be actively resolved.
- Relationships and culture: zero-tolerance policies on bullying and harassment that are actually enforced, not simply documented. Psychological safety, the sense that speaking up will not be punished, is a significant protective factor.
- Change management: informing employees about proposed changes early, explaining the rationale, involving them where possible, and providing support during transition. Change that feels arbitrary and opaque generates disproportionate anxiety.
Secondary Interventions: Building Resilience
Secondary interventions strengthen the individual's capacity to manage unavoidable pressure. They are valuable but should not be deployed as a substitute for primary intervention.
- Mental health awareness training for managers: equipping line managers to recognise the signs of stress in their teams, to have early conversations, and to signpost appropriately. This is consistently one of the highest-return investments an organisation can make.
- Mental health first aid training: qualifying members of staff in recognised mental health first aid gives organisations trained individuals who understand the principles of early intervention, active listening, and referral.
- Stress management skills for employees: practical techniques covering time management, assertiveness, boundary-setting, and physiological self-regulation.
- Mindfulness-based programmes: there is solid evidence for mindfulness-based stress reduction (MBSR) in reducing self-reported stress and improving sleep quality.
Tertiary Interventions: Support and Recovery
Tertiary interventions are essential for employees who are already unwell, but their purpose is to support recovery rather than to serve as the only strategy.
- Employee Assistance Programmes (EAPs): confidential access to counselling, financial advice, and legal guidance. Engagement rates are often low; actively promoting these services and reducing stigma around their use is important.
- Phased return to work: structured, supported return following stress-related absence, with a review of the conditions that contributed and adjustments made where possible.
- Occupational health referral: professional assessment of fitness for work and recommendations for workplace adjustments.
- Manager support during long-term absence: regular, non-pressuring contact that maintains the employee's connection with the organisation.
£4.70
Average return per £1 invested in workplace mental health (Deloitte, 2024)
Based on a literature review of 26 studies since 2011 reporting financial returns on workplace wellbeing interventions
Mental Health First Aid: Building Organisational Capacity
Organisations looking for a practical, structured way to improve their response to stress and mental ill health should consider training mental health first aiders. Just as a physical first aider is trained to recognise and respond to physical health emergencies, a mental health first aider is trained to recognise the early signs of mental ill health, to provide initial non-clinical support, and to guide the individual towards appropriate professional help where needed. The role is not that of a counsellor or clinician: it is the organisational equivalent of the person who spots a problem early and knows what to do next.
Having trained mental health first aiders in an organisation serves several purposes. It normalises conversations about mental health, provides a visible point of contact for employees who are struggling before difficulties escalate, and reduces the time between a person experiencing difficulties and receiving appropriate support. Critically, it complements rather than replaces the legal duty to conduct a risk assessment: first aiders are the human infrastructure that responds to what the assessment identifies. Organisations where the two exist together are better placed than those relying on either alone.
A Practical Checklist for Employers
Based on the evidence and legal requirements set out above, the following represents a minimum framework for responsible stress management in a UK workplace.
| Action | Notes |
|---|---|
| Conduct a formal assessment of psychosocial risks | Use the HSE Management Standards approach and Stress Indicator Tool. Document findings. Review at least annually and after significant organisational change. |
| Analyse sickness absence data by team and role | Stress-related absence clustered in specific areas usually indicates a management, workload, or culture issue rather than individual fragility. |
| Train line managers in mental health awareness | Managers who cannot recognise stress or have not developed the skills to discuss it are themselves a significant risk factor. |
| Establish clear communication about change | Before, during and after any significant change. Silence generates anxiety at least as damaging as difficult news delivered clearly. |
| Review workload and role clarity | Ensure job descriptions reflect reality. Address role conflict directly. Have honest conversations about capacity. |
| Promote support mechanisms actively | EAPs, occupational health, and mental health first aiders are only useful if people know about them and trust that using them will not affect their career. |
| Consider mental health first aid training | Qualify trained individuals at RQF Level 2 or 3 to provide structured initial support and appropriate signposting. |
| Create psychological safety | People will not report stress if they believe doing so will harm them. Leaders model this by talking openly about pressure and demonstrating that candour is safe. |
The Bottom Line
Stress is not a character flaw or a sign of weakness. It is a physiological response, shaped by millions of years of evolution, that becomes harmful when it runs without relief in environments it was never designed for. Modern working life, with its chronic low-grade pressures, its always-on culture, and its frequent disconnect between effort and control, is particularly adept at triggering that response.
The organisations that manage stress effectively are not those with the most elaborate wellness programmes. They are those that take seriously the question of how work is designed: whether demands are reasonable, whether people have genuine control over their work, whether support is real rather than nominal, and whether the culture makes it safe to say so when something is wrong.
That is within reach of any organisation prepared to look honestly at the evidence, meet its legal obligations, and treat psychological health with the same rigour it would apply to any other workplace risk.

Ready to Build a Stress-Resilient Workplace?
Constellation Training delivers Ofqual-regulated mental health and workplace wellbeing qualifications across the UK. Whether you need a Mental Health First Aid course for your team, mental health awareness training for managers, or a bespoke in-house programme, we can help.
If your organisation needs First Aid for Mental Health training, you can discuss your requirements here.
References
1. Health and Safety Executive. Work-related stress, depression or anxiety statistics in Great Britain 2025. hse.gov.uk/Statistics/assets/docs/stress.pdf [Published November 2025, accessed March 2026]
2. Deloitte UK. Mental Health and Employers: The Case for Investment (4th edition). deloitte.com/uk, May 2024.
3. Mental Health Foundation / London School of Economics and Political Science. The Economic and Social Costs of Mental Health Problems. 2024.
4. Mental Health UK / YouGov. Burnout Report 2025. mentalhealth-uk.org [Accessed March 2026]
5. Goldstein DS. Evolution of concepts of stress. Stress. 2007;10(2):109-120. doi:10.1080/10253890701288935
6. Cannon WB. Organization for physiological homeostasis. Physiological Reviews. 1929;9:399-431.
7. Tan SY, Yip A. Hans Selye (1907-1982): Founder of the stress theory. Singapore Medical Journal. 2018;59(4):170-171. PMC5915631.
8. Selye H. Stress without Distress. New York: Signet; 1975.
9. Goldstein DS. Evolution of concepts of stress. Stress. 2007;10(2):109-120.
10. World Health Organization. Burn-out an "occupational phenomenon": International Classification of Diseases. who.int 2019.
11. Health and Safety Executive. Management Standards for Tackling Work-Related Stress. hse.gov.uk/stress/standards/ [Accessed March 2026]
12. Health and Safety Executive. Work-related stress, depression or anxiety statistics in Great Britain 2025. hse.gov.uk [Published November 2025]
13. Health and Safety Executive. Work-related stress, depression or anxiety statistics in Great Britain 2025: age and gender breakdown. hse.gov.uk/Statistics/assets/docs/stress.pdf [Published November 2025]
14. Health and Safety at Work etc. Act 1974. Section 2. legislation.gov.uk
15. Management of Health and Safety at Work Regulations 1999. Regulation 3. legislation.gov.uk
16. Equality Act 2010. Section 6. legislation.gov.uk



